Uploaded by
gencselim
Refractive and Corneal Aberrometric Changes After Crescentic Lamellar Wedge Resection in Pellucid Marginal Degeneration

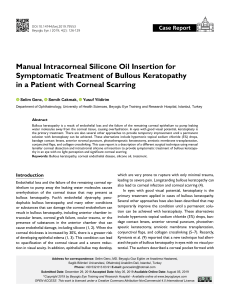
ARTICLE Refractive and Corneal Aberrometric Changes After Crescentic Lamellar Wedge Resection in Pellucid Marginal Degeneration Selim Genç, M.D., Hanefi Çakır, M.D., Objective: To evaluate the effectiveness of crescentic corneal lamellar wedge resection for the treatment of pellucid marginal degeneration (PMD) in improving refractive, visual, and corneal aberrometry. Methods: The study included 10 eyes of 10 patients who had undergone corneal lamellar wedge resection for PMD. Pellucid marginal degeneration was diagnosed based on the clinical signs and corneal topography. The corneal aberrometry was evaluated with Sirius corneal topography. Results: The mean follow-up period was 14.1 months (range, 9–24 months). Uncorrected visual acuity was improved in nine eyes and remained unchanged in 1 case, whereas best-corrected visual acuity was improved in all eyes postoperatively. By vector analysis, the overall mean astigmatic drift at the last visit was calculated to be 13.066.3 diopters (D). At last visit, significant reductions were found for all aberrometric measurements. However, the differences were not significant for the measurements of trefoil (P¼0.189). Conclusions: Corneal lamellar wedge resection is a favorable surgical option for management of PMD, allowing for improved visual acuity, keratometric cylinder, and corneal aberrations. Key Words: Crescentic corneal lamellar wedge resection—Pellucid marginal degeneration—Corneal aberrometry. (Eye & Contact Lens 2017;0: 1–5) P ellucid marginal degeneration (PMD) is an ectatic corneal disease, which is generally associated with a crescent shape of inferior peripheral corneal thinning.1 The ectatic corneal morphology causes against-the-rule astigmatism and visual loss.2 The management of PMD includes a variety of treatment modalities— spectacles, rigid gas-permeable contact lenses,3 and surgical techniques such as intracorneal ring segments,4 full-thickness crescentic wedge resection,5 lamellar crescentic wedge resection,6 deep anterior lamellar keratoplasty,7 and penetrating keratoplasty (PK).8 Intracorneal ring segments are inadequate to decrease high levels of astigmatism and may not eliminate corneal ectasia, which is From the Department of Ophthalmology (S.G.), Lütfi Kırdar Kartal Eye _ Training and Research Hospital, Istanbul, Turkey; Eye Clinic (H.C., E.G.), _ Türkiye Hospital, Istanbul, Turkey; and Department of Ophthalmology (Ü. _ Ç.), Ümraniye Training and Research Hospital, Istanbul, Turkey. The authors have no funding or conflicts of interest to disclose. Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal’s Web site (www. eyeandcontactlensjournal.com). Address correspondence to Emre Güler, M.D., Türkiye Hospital, Merkez _ Mah. Darülacaze Cad. No: 14/1, 34381 Şişli/Istanbul, Turkey; e-mail: [email protected]. Accepted May 27, 2017. DOI: 10.1097/ICL.0000000000000409 Eye & Contact Lens Volume 0, Number 0, Month 2017 Emre Güler, M.D., and Ümit Çallı, M.D. probably associated with disease progression. Full-thickness wedge resection and PK include open eye surgery risks and may be associated with glaucoma due to the marginal location and extend of the graft.9 The advantages of crescentic lamellar wedge resection include the removal of pathological tissue which improves the corneal morphology and irregular astigmatism without the use of allogeneic tissue and risks of open eye surgery.10 Wavefront technology has been used for the measurement of ocular or corneal higher-order aberrations (HOAs) which are uniquely described by a weighted sum of the Zernike terms.11 In PMD, the increased corneal HOAs, especially the trefoil and spherical aberrations, are the leading causes of optical errors along with the induced against-the-rule astigmatism and visual acuity decline.12 In this study, we aimed to evaluate the refractive, visual, and corneal aberrometric changes after lamellar crescentic wedge resection in eyes with PMD. To the best of our literature knowledge, this is the first study to analyze the corneal aberrometric changes after lamellar crescentic wedge resection in PMD. PATIENTS AND METHODS Ten eyes of 10 patients with PMD who underwent lamellar crescentic wedge resection at our institutions between November 2013 and January 2015 were evaluated retrospectively. Included patients had steep keratometry .57 D, best-corrected visual acuities (BCVAs) between 20/40 and 20/400, and intolerance to spectacle or contact lens use. Excluded patients had a history of ocular surgery, ocular trauma, and any ocular disease other than PMD. The study patients had provided their informed consent. The study was conducted in accordance with the ethical standards stated in the Declaration of Helsinki and was approved by the Local Ethics Committee. Pellucid marginal degeneration was diagnosed based on the findings of slit-lamp biomicroscopy (corneal ectasia localized inferiorly along with corneal thinning), corneal topography (butterfly pattern, high steep contour, and increased keratometric powers radiating toward the inferior peripheral cornea), and refractive changes (convincing against-the-rule astigmatism along with a decline of BCVA). All eyes had a comprehensive preoperative and postoperative ophthalmic examination that included uncorrected visual acuity (UCVA), BCVA, manifest refraction by autorefraction (TOPCON), intraocular pressure (IOP), slit-lamp biomicroscopy, and corneal topography with Orbscan (Oculus Optikgeräte GmbH, Wetzlar, Germany) and Sirius (Costruzione Strumenti Oftalmici, Florence, Italy) devices. Visual acuity was measured with Snellen charts and converted to logarithm of the minimal angle of 1 Copyright Contact Lens Association of Opthalmologists, Inc. Unauthorized reproduction of this article is prohibited. Eye & Contact Lens Volume 0, Number 0, Month 2017 S. Genç et al. keratometric powers and corneal wavefront values. The SE was the sum of the spherical and half of the cylindrical values. The vector analysis demonstrated the degree of the astigmatic correction which includes the final amount of astigmatism and change in astigmatism achieved by surgery.13,14 resolution values. Corneal wavefront analysis was performed in eight eyes using Sirius device which uses a monochromatic rotating Scheimpflug camera and a Placido disk. The Sirius performs the aberrometric measurements by the ray-tracing technique. The corneal wavefront measurements including the root mean square (RMS) values of HOAs, coma, trefoil, and spherical aberrations were obtained over a 6-mm optical zone and decomposed into Zernike polynomials to the sixth order. Data Analysis SPSS 21.0 for Windows (SPSS Inc., Chicago, IL) was used for the statistical analysis. The distribution of the data was normal and met by the Kolmogorov–Smirnov test (P.0.05). The measured variables were evaluated by Wilcoxon signed-rank test. P value less than 0.05 was accepted to be statistically significant. Surgical Technique The surgical procedures were applied using peribulbar anesthesia. Initially, the borders of the area to be excised were signed using a gentian violet under the operating microscope. We aimed to prepare a corneal tissue with 10-mm length and 1.5-mm width centrally. Using a 45° metal blade, a crescentic wedge of ectatic corneal tissue (with a deepening of at least 80% of corneal thickness) was excised in each case. After wedge resection, anterior chamber paracentesis was performed using a 1.2-mm single-plane side-port incision to provide intraocular hypotony, and then the wound resulting from wedge resection was sutured with 10-0 nylon suture. Initially, a central suture was applied and was continued one by one in each side (see Video, Supplemental Digital Content 1, http://links.lww.com/ICL/A62). Postoperative regimen included moxifloxacin and dexamethasone eyedrops which were applied 5 times a day for a 4-week period. Main outcome measures were UCVA, BCVA, spherical equivalent (SE) refraction, and corneal topography findings including TABLE 1. RESULTS The study included six men and four women. The mean age of patients was 54.467.3 years (range 41–73 years). The mean follow-up period was 14.164.9 months (range, 9–24 months). All patients had inferior thinning. Table 1 demonstrates the preoperative and postoperative data of the patients. The mean UCVA and BCVA were significantly improved postoperatively (P were ,0.001 and 0.001, respectively). Uncorrected visual acuity was improved in nine eyes and remained unchanged in 1 case (case 10, Table 1), whereas BCVA was improved in all eyes postoperatively. All patients had improved BCVA with spectacles. Preoperative and Postoperative Refractive Outcomes UCVA, logMAR BCVA, logMAR SE, D Patient Preoperative Postoperative Preoperative Postoperative Preoperative Postoperative 1 2 3 4 5 6 7 8 9 10 Mean SD P 2.0 1.3 1.0 1.3 1.3 1.5 1.5 2.0 2.0 2.0 1.59 0.38 1.0 0.5 0.4 0.7 0.7 0.5 0.8 1.0 1.8 2.0 0.95 0.54 ,0.001 1.3 0.4 0.3 0.7 0.8 0.7 0.7 1.0 2.0 0.4 0.83 0.50 0.2 0.1 0.1 0.2 0.1 0.2 0.3 0.4 0.5 0.2 0.23 0.13 0.001 27.75 25.75 210.0 27.87 211.50 28.62 21.75 27.12 NA NA 26.03 4.09 24.12 20.25 23.62 21.87 25.12 0.75 1.62 23.75 21.50 22.25 22.01 2.21 0.006 SimK, D Keratometric Cyl, D Patient Preoperative Postoperative Preoperative Postoperative Vector Change in Keratometric Cyl, D Follow-up, mo 1 2 3 4 5 6 7 8 9 10 Mean SD P 53.20 51.97 55.86 56.66 50.74 51.78 48.44 51.91 55.40 43.50 51.94 3.88 50.40 41.04 44.29 52.03 46.24 44.87 42.64 43.38 45.30 46.20 45.63 3.36 0.001 2.2·156 9.9·11 9.9·26 10.4·11 9.4·166 8.9·176 3.3·152 7.7·133 6.2·167 13.7·171 8.1 3.4 1.2·70 7.1·90 7.7·93 9.9·85 6.8·97 4.3·64 4.8·95 7.3·120 15.3·90 5.2·120 7.0 3.7 0.169 3.5 16.7 16.3 19.6 15.2 12.3 6.9 3.4 21.0 15.6 13.0 6.3 18 24 12 9 15 18 9 12 18 10 14.15 4.94 P,0.05 indicates statistically significant intragroup difference. BCVA, best-corrected visual acuity; Kf, keratometry flat; Kf, keratometry steep; logMAR, logarithm of the minimal angle of resolution; NA, Not Applicable; SE, spherical equivalent; SimK, simulated keratometry; UCVA, uncorrected visual acuity. 2 Eye & Contact Lens Volume 0, Number 0, Month 2017 Copyright Contact Lens Association of Opthalmologists, Inc. Unauthorized reproduction of this article is prohibited. Eye & Contact Lens Volume 0, Number 0, Month 2017 Because of advanced ectasia, we managed to assess SE values for eight of all eyes. For these eyes, the mean SE was 26.0364.09 D preoperatively and 22.0162.21 D postoperatively (P¼0.006). The mean preoperative simulated keratometry was 51.9463.88 D, and at last visit, it was significantly reduced to 45.6363.36 D (P¼0.001). The mean preoperative keratometric cylinder was 8.163.4 D, and at the last visit, it was improved to a postoperative mean of 7.063.7 D (P¼0.169). By vector analyzes, the overall mean astigmatic drift was calculated to be 13.066.3 D at the last visit (Fig. 1). A detailed data of the corneal aberrometric values is shown in Table 2. At the last visit, significant reductions were found for all aberrometric measurements. However, the differences were not significant for the measurements of trefoil (P¼0.189). Intraoperative corneal microperforation occurred in one patient, and it was sutured simultaneously with the absence of postoperative sequelae (Fig. 2). Descemet membrane striae occurred in all cases; however, none of these were present in the central cornea and caused irregular astigmatism. In addition, during follow-up period, no cases had increased IOP or recurrence of PMD. The selective suture removal time was at least 6 months, and three eyes had still sutures remaining at last review. DISCUSSION Many authors have reported resection of a wedge shaped ectatic corneal tissue in PMD.5,10,15,16 This surgical approach provides many advantages superior to penetrating methods which include the conservation of normal central cornea, mechanically stronger wound, faster visual recovery, and the absence of steroid-related adverse effects or immunologic rejection.5,17 The primary purpose of this surgical procedure is to remove the ectatic corneal tissue, provide a normal corneal structure, and prevent the progression of the disease. Full-thickness crescentic wedge resection includes the risks open eye surgery and glaucoma. To avoid these complications, deep lamellar dissection as close as possible to the Descemet Aberrometric Changes in PMD membrane is crucial and to obtain a smooth surface which prevents striae, interface opacification, and irregular astigmatism. Limited number of studies evaluated the efficacy of the lamellar crescentic wedge resection in the management of PMD. Busin et al.16 performed lamellar wedge resection combined with penetrating relaxing incisions in 10 eyes with PMD. The BCVA improved in eight patients, and the mean keratometric astigmatism was reduced from 15.1 D preoperatively to 4.6 D at 6 months postoperatively. Maccheron et al.10 showed improvement in BCVA along with a 9.1 D reduction in keratometric cylinder at postoperative 10 months in seven eyes with PMD. Similar to previous studies, corneal shape and astigmatism were favorably corrected along with a significant gain in UCVA and BCVA using lamellar corneal wedge resection technique. In general, a mild corneal flattening was induced by the surgery, which resulted in a decrease in corneal keratometry and hyperopic alteration in SE postoperatively. MacLean et al.5 reported the outcomes of full-thickness crescentic wedge resection in 10 eyes with PMD. Postoperatively, an improvement in BCVA was achieved in all eyes. Mean keratometric astigmatism decreased from 13.8 D to 1.4 D. However, astigmatic drift was noted at long-term follow-up with a mean of 2.1 D (range 0.5–5.5 D). In addition, three patients showed inferior pannus associated with sutures, and 1 case had corneal hydrops in the corneal wound postoperatively. In our cases, no patient had astigmatic drift, corneal vascularization, and suture-related complications. A few studies have discussed HOAs in patients with PMD. Kamiya et al.18 reported an increased corneal coma-like aberration while the spherical-like aberration did not change in the 11 year follow-up of a case with PMD. The features of ocular HOAs in eyes with PMD using Zernike terms were evaluated only in one study.12 They found significantly increased corneal HOAs compared with healthy eyes with the mean total HOA RMS of 0.5660.28 mm, coma of 0.2760.19 mm, and spherical aberration of 0.08660.10 mm. In the current study, the corneal aberrations FIG. 1. (A) The preoperative topography of case 2. (B) The same case at 24 months postoperatively showing a 16 D improvement in astigmatism. 2017 Contact Lens Association of Ophthalmologists 3 Copyright Contact Lens Association of Opthalmologists, Inc. Unauthorized reproduction of this article is prohibited. Eye & Contact Lens Volume 0, Number 0, Month 2017 S. Genç et al. TABLE 2. Preoperative and Postoperative Mean Square (RMS) Results of Corneal Wavefront Aberrations HOA, mm (Mean 6 SD) Coma, mm (Mean 6 SD) Trefoil, mm (Mean 6 SD) Spherical, mm (Mean 6 SD) Patient Preoperative Postoperative Preoperative Postoperative Preoperative Postoperative Preoperative Postoperative 1 2 3 4 5 6 7 8 Mean SD P 6.26 4.32 6.15 4.82 5.50 8.39 2.90 3.72 5.25 1.71 4.91 3.83 5.45 4.22 2.28 3.22 1.15 2.45 3.43 1.44 0.015 5.35 8.32 4.50 2.19 4.83 6.04 2.68 3.19 4.63 2.00 4.05 3.42 3.45 1.17 3.16 2.88 1.18 1.86 2.64 1.10 0.004 2.29 6.23 0.89 3.26 1.65 8.54 0.76 1.61 3.15 2.79 2.27 0.84 1.17 3.19 1.88 2.28 1.12 1.18 1.74 1.80 0.189 21.71 21.75 22.97 22.04 21.69 21.54 20.44 20.33 21.55 0.85 20.40 0.28 0.02 20.56 20.28 20.22 20.12 20.08 20.17 0.25 0.003 P,0.05 indicates statistically significant intragroup difference. HOA, higher-order aberration; RMS, root mean square. were considerably higher in our cases than the previously reported as shown in Table 2. It has been shown that the progression in topographic changes induce high degrees of against-the-rule astigmatism and coma-like aberrations.18 In routine clinical practice, corneal aberrations should be considered when evaluating the optical quality. In eyes with PMD, the increased corneal aberrations are one of the leading causes of optical deficits. To the best of our literature knowledge, the current study is the first to assess the corneal aberrometry after lamellar crescentic wedge resection in PMD. In our cases, higherorder, coma-like, and spherical-like aberrations were significantly decreased postoperatively. Furthermore, trefoil also showed a decrease; however, it was not statistically significant. The early goal of this surgical method is to provide an overcorrection in corneal astigmatism which regresses by corneal remodeling, wound healing, and suture loosening in the postoperative period. Further management of astigmatism can be achieved by selective suture removal or controlling of corneal wound healing by topical steroid usage. Therefore, the visual rehabilitation after lamellar wedge resection involves a long period. In our cases, the time for selective suture removal was at least 6 months postoperatively, and spectacles were used for visual rehabilitation at the earliest opportunity. In this study, we have excised a longer wedge shaped corneal tissue (10 mm) to achieve homogenous corneal flattening and normalize the inferior–superior meridian of the cornea. In addition, anterior chamber paracentesis should be performed to provide intraocular hypotony. This allows the in folding of the Descemet membrane and edge-to-edge suturing of the stromal wounds which enhances the effectiveness of the surgery. Wedge resection may also be useful to provide an appropriate corneal bed for further corneal transplantation. Wedge resection, especially when involves a large amount of corneal tissue followed by simple closure of wound, may cause Descemet membrane striae formation and irregular astigmatism. To prevent this complication, lamellar dissection and/or relaxing incisions may be considered. In our study, a large amount of corneal tissue has been excised (1.5-mm width centrally); however, because of its crescent shape, resection acts as a relaxing incision in the peripheral cornea. In all cases, Descemet membrane striae occurred; however; none of these were present in the central cornea and caused irregular astigmatism. In conclusion, lamellar crescentic wedge resection is a favorable surgical option to improve the visual acuity and astigmatism in advanced PMD which directly targets the corneal ectasia without the risks of allograft PK and lamellar keratoplasty. Furthermore, corneal HOAs are significantly improved after this surgery. Future studies of the outcomes with lamellar crescentic wedge resection in corneas with PMD in the long term are required to confirm our findings. ACKNOWLEDGMENTS The authors thank Prof. Sait E g rilmez for statistical analysis. REFERENCES FIG. 2. Slit-lamp photography shows the postoperative appearance of a successful excision of a thinned area of cornea at postoperative 3 months. 4 1. Sridhar MS, Mahesh S, Bansal AK, et al. Pellucid marginal corneal degeneration. Ophthalmology 2004;111:1102–1107. 2. Karabatsas CH, Cook SD. Topographic analysis in pellucid marginal corneal degeneration and keratoglobus. Eye (Lond) 1996;10:451–455. 3. Kompella VB, Aasuri MK, Rao GN. Management of pellucid marginal corneal degeneration with rigid gas permeable contact lenses. CLAO J 2002;28:140–145. 4. Barbara A, Shehadeh-Masha’our R, Zvi F, et al. Management of pellucid marginal degeneration with intracorneal ring segments. J Refract Surg 2005; 21:296–298. Eye & Contact Lens Volume 0, Number 0, Month 2017 Copyright Contact Lens Association of Opthalmologists, Inc. Unauthorized reproduction of this article is prohibited. Eye & Contact Lens Volume 0, Number 0, Month 2017 5. MacLean H, Robinson LP, Wechsler AW. Long-term results of corneal wedge excision for pellucid marginal degeneration. Eye (Lond) 1997;11 (Pt 5):613–617. 6. Javadi MA, Karimian F, Hosseinzadeh A, et al. Lamellar crescentic resection for pellucid marginal corneal degeneration. J Refract Surg 2004;20: 162–165. 7. Millar MJ, Maloof A. Deep lamellar keratoplasty for pellucid marginal degeneration: Review of management options for corneal perforation. Cornea 2008;27:953–956. 8. Tzelikis PF, Cohen EJ, Rapuano CJ, et al. Management of pellucid marginal corneal degeneration. Cornea 2005;24:555–560. 9. Williams KA, Lowe M, Bartlett CM, et al. The Australian Corneal Graft Registry Report 2007. Adelaide, Australia: Flinders University Press, 2007. 10. Maccheron LJ, Daya SM. Wedge resection and lamellar dissection for pellucid marginal degeneration. Cornea 2012;31:708–715. 11. Thibos LN, Hong X. Clinical applications of the Shack-Hartmann aberrometer. Optom Vis Sci 1999;76:817–825. 2017 Contact Lens Association of Ophthalmologists Aberrometric Changes in PMD 12. Oie Y, Maeda N, Kosaki R, et al. Characteristics of ocular higher-order aberrations in patients with pellucid marginal corneal degeneration. J Cataract Refract Surg 2008;34:1928–1934. 13. Miller JM. Clinical applications of power vectors. Optom Vis Sci 2009;86: 599–602. 14. Egrilmez SDG, Yagci A. Vector analysis Software on analyzing astigmatism. Turk J Ophthalmol 2003:404–416. 15. Biswas S, Brahma A, Tromans C, et al. Management of pellucid marginal corneal degeneration. Eye (Lond) 2000;14:629–634. 16. Busin M, Kerdraon Y, Scorcia V, et al. Combined wedge resection and beveled penetrating relaxing incisions for the treatment of pellucid marginal corneal degeneration. Cornea 2008;27:595–600. 17. Varley GA, Macsai MS, Krachmer JH. The results of penetrating keratoplasty for pellucid marginal corneal degeneration. Am J Ophthalmol 1990; 110:149–152. 18. Kamiya K, Hirohara Y, Mihashi T, et al. Progression of pellucid marginal degeneration and higher-order wavefront aberration of the cornea. Jpn J Ophthalmol 2003;47:523–525. 5 Copyright Contact Lens Association of Opthalmologists, Inc. Unauthorized reproduction of this article is prohibited.


![[David Seal, Uwe Pleyer] From Paradise To Paradigm(BookFi) cennetten paradigmaya](http://s2.studylibtr.com/store/data/005902225_1-3ad24fc5a2423e6802f8ebdfdcc686e0-300x300.png)