Uploaded by
common.user3977
Chick Embryo CAM: In Vivo Wound Healing Model

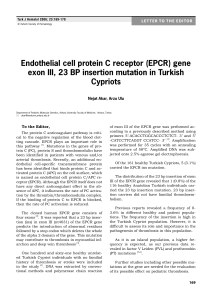
Path. Res. Pract. 192, 1068-1076 (1996) The Chick Embryo Chorioallantoic Membrane as an in vivo Wound Healing Model D. Ribatti\ A. Vacca 2 , G. Ranieri 2 , S. Sorino1 and L. Roncalj1 11nstitute of Human Anatomy, Histology and Embryology, 2Department of Biomedical Sciences and Human Oncology, University of Bari Medical School, Bari, Italy SUMMARY The chick embryo chorioallantoic membrane (CAM) was used as an in vivo wound healing model. A full excision of a 1 mm 2 CAM area was filled by a granulation tissue after 96-120 h, which eventually formed a scar in 75% of the cases. In the remaining 25%, a solution of continuity was left which, however, was smaller in size than the One observed immediately after the excision. Under the microscope, the CAM area involved in the repair process showed: i. hyperplasia of the chorionic epithelium; ii. about three times as many microvessels and fibroblasts in the mesenchyme as in the normal adjacent control regions; iii. an inflammatory infiltrate mostly consisting of macrophages; and iv. a strong positivity for fibronectin in the extracellular matrix. The validity of this experimental model appears to be confirmed by the fact that we were able to reproduce all the critical events controlling the wound healing process, such as re-epithelization, angiogenesis, formation of an inflammatory infiltrate and deposition of one of the main constituents of the extracellular matrix, such as fibronectin. Introduction Wound healing (WH) is characterized by the formation of a granulation tissue consisting of inflammatory cells, newly-formed blood vessels and fibroblasts embedded in a loose collagenous extracellular matrix. Re-epithelization, angiogenesis and matrix deposition are critical events controlling this process 8• Angiogenesis is confined to the wound site 1 and plays a pivotal role for successful WHo Revascularization is required to furnish the new tissue and metabolities, and to dispose of the waste products of metabolism. Angiogenesis occurs as a higher regulated process which is rapidly stimulated after injury and ceases when WH is complete l2 • 0344-0338/96/0192-1068$3.50/0 Extracellular matrix proteins are known to be important in many phases of WH. Among these proteins, fibronectin, a glycoprotein secreted by proliferating endothelial cells ,21, forms the provisional extracellular matrix of wounds 14,19 and promotes migration of endothelial cells over the wound 27• A frequently employed method to stimulate WH in vivo is the subcutaneous implantation of sponges 9 • In this work, we examined the modes of WH development in an experimentally induced lesion in the chick embryo chorioallantoic membrane (CAM). Specifically, we examined WH with respect to the amount of the associated vasoproliferative processes, the characteristics of the inflammatory infiltrate and of the extracellular matrix adjacent to the site of the lesion. Our © 1996 by Gustav Fischer Verlag, Stuttgart The CAM as an in vivo Wound Healing Model· 1069 Table 1. Quantitation of microvessels in the CAM's intermediate mesenchyme Under the wound Distant from the wound (Control) Microvessel density (%)a No. of intersection points b 11.2 3.3 54.5±5.2 C 16.2±1.6 a For specification see text, b Mean ± SD, C Statistically significant difference p < 0.001 vs number of intersection points distant from the wound. Table 2. Quantitation of fibroblasts in the CAM's intermediate mesenchyme Under the wound Distant from the wound (Control) Fibroblast density(%)a No. of intersection points b 16.5 5.2 80.4±12.5 C 25.2±6.3 a For specification see text, b Mean+SD, C Statistically significant difference p < 0.001 vs number of intersection points distant from the wound. findings suggest that CAM can be regarded as an in vivo WH model. Results Macroscopic Examination The CAM region surrounding the continuity solution showed swift vasoproliferative processes as early as 24 h after excision (HH stage 36) (Fig.1a). In 75% of the cases, the solution of continuity was filled by a granulation tissue within 48 to 72 h (HH stages 37-3 8). The scar developed upon this tissue during the next 24-48 h (HH stages 39-40) (Fig.1b). In the remaining 25% of the specimens, a solution of continuity smaller than the initial one was still present. Microscopic Examination Where the macroscopic examination showed that the solution of continuity had been filled by granulation tissue, the histologic examination confirmed that CAM continuity had been fully restored. Conversely, when a macroscopic analysis revealed that the continuity solution had only been filled by the scar tissue, an optical empty space between the two juxtaposed CAM stumps (Fig.2a) could be observed under the microscope. The chorionic epithelium of the stumps, normally consisting of 1 or 2 cell layers, was here formed by 2 to 6 layers (Fig.2 a-c). Within 96120 h following the lesion, microvessels and fibroblasts density in the underlying mesenchyme was about three times as high as in the adjacent normal control regions (Fig. 2 b, c Tables 1, 2}. The mesenchyme also showed the presence of an inflammatory infiltrate, mostly distributed in a perivascular position (Fig. 2 d} and consisting prevailingly of macrophages that reacted positively to naphthol-AS-D-chloroace- tate esterase activity. Under normal conditions these cells are located almost exclusively inside the vessels (Fig.3 a); instead, where the lesion had been performed experimentally, their location was mostly interstitial (Fig. 3 b). Lastly, the extracellular matrix reacted with fibronectin in the mesenchyme beneath the lesion. Fibronectin deposition started 24 h after the lesion had been produced and reached its maximum extension after 24-48 h (Fig.4). Discussion In this work, we have followed the time-course of the repair process of an experimentally induced wound in the chick embryo CAM. In 75% of the cases, a 1 mm 2 resection area forms a scar some 96 -120 h later. The scar itself consists of a granulation tissue formed by newly-formed vessels, fibroblasts and inflammatory infiltrate essentially composed of macrophages. The process of WH depends upon a variety of interactions between cells and the extracellular matrix components, and wound repair is in part mediated by multiple growth factors released by inflammatory cells and from their storage sites of the extracellular matrix. In the CAM mesenchyme beneath the lesion we demonstrated that the number of microvessels was three times higher than in the normal adjacent regions which were considered as the control. WH angiogenesis has been extensively studied 1,22 and is characterized by disruption of the integrity of endothelial cell monolayers in pre-existing microvessels, basement membrane lysis, endothelial migration and proliferation, lumen and capillary loop formation. Angiogenesis is an absolute requirement for the development of the granulation tissue during WH. For example, under the category of wound repair the healing of peptic ulcers and of myocardial infarction is dependent upon angiogenesis 11. Healing is accelerated by the use of exogenous angio- 1070 . D. Ribatti et al. * -. a b. Fig. 1 a - b a: 1O-day old CAM (HH stage 36), 24 h after a full thickness excision of a small CAM's area (asterisk). The margins of the lesion show an intense vasoproliferative response - b: 14-day old CAM (HH stage 40), 120 h after the excision. The solution of continuity has been filled by a scar tissue (arrows). Original magnifications: a, x30; b, x20. The CAM as an in vivo Wound Healing Model· 1071 , r, f a Fig. 2 a-d. Light micrographs showing in (a) an optically empty space (arrow) between the two juxtaposed CAM stumps of an experimental case in which continuity solution had been partially filled by the scar tissue. Note in (b, c) the two stumps photographed at higher magnification showing the hyperplasia of the chorionic epithelium (C) with the increase of vessels and fibroblasts in the underlying mesenchyme (M), and in (d) inflammatory cells located in perivascular position. Original magnifications: a, x 100; b, d, x400; c, x250. 1072 . D. Ribatti et al. Fig. 2c, d. The CAM as an in vivo Wound Healing Model· 1073 .a", 06 • • ~"-t :.J! ,,: ' • ~, ,\ w. 0 ~ 0 ".I+f ,'", 11-. • f', <;" .. to .• . .... ~ ~o • '. ... ',,' 1! . Fig. 3 a-b. Naphtol-AS-D-chloroacetate esterase positive cells in a control (a) and an experimental (b) case. In (a) the cells are prevalently located inside the vessels; in (b) they are outside, in the CAM's mesenchyme. Original magnifications: a, b, x2S0. 1074 . D. Ribatti et al. Fig. 4. CAM's immunoperoxidase staining using a mAB to the fibronectin, in an experimental case in which CAM's continuity solution had been completely filled by the scar tissue. Note, on the left, in the mesenchyme (M) underlying the chorionic epithelium (C), a immunoreactivity (arrowhead) condensed in some areas of the epithelium-connective interface. Original magnification: x150. genic factors 4, 5, 23. In contrast, when neovascularization is suppressed or delayed, WH itself is retarded 2 ,25. Simultaneously with the increase in vascular density, we also demonstrated in the CAM mesenchyme about three times as many fibroblasts as in the contiguous control regions. Hence, fibroblasts participate in large numbers in the formation of the granulation tissue during the WH process. There is possibly a close relationship between the increase in vascular density and the number of fibroblasts. Recently, a transformation of fibroblasts into endothelial cells during angiogenesis has been demonstrated 18. Moreover, co-cultures of endothelial cells and fibroblasts in collagen gels elicited an angiogenic response as demonstrated by the reorganization of endothelial cells into a capillary-like network with lumens 2o • An adequate stimulus for fibroblasts multiplication could be represented by the basic fibroblast growth factor (bFGF) released by the macrophages 22 ,30. In our work, these cells represent the main cell population in the inflammatory infiltrate, which in turn participates in the composition of the granulation tissue and shows an interstitial arrangement instead of the intravascular distribution observed under normal conditions. Macrophages are another source of angiogenic activity in a WHo They migrate in the depth of a wound where oxygen tension is very low l6 , a condition stimulating these cells to release angiogenic factors, including bFGF, transforming growth factors (TGF-a and -Pl, granulocyte-macrophage colony stimulating factor (GM-CSF), vascular endothelial growth factor (VEGF), interleukin-8 (IL-8) and tumor necrosis factor alpha (TNF-a)22,30. lt is of note that WH is delayed when transformation of monocyte into macrophage is prevented by corticosteroids 13. Angiogenic factors, such as bFGF, could be mobilized from the CAM extracellular matrix strores 29 by the proteases released by the endothelial cells. We also demonstrated a marked positivity for fibronectin in the extracellular matrix underlying the lesion during the granulation tissue formation process. Cells forming granulation tissue, such as macrophages, produce fibronectin deposited into the tissue matrix l9 • Proliferating endothelial cells also synthesize and secrete fibronectin in vivo 3, 21 and increased fibronectin appears in dermal blood vessels exhibiting endothelial cell proliferation during delayed type hypersensitivity reactions 6 • In addition, fibronectin derived from extravased plasma increases markedlr after injury and supports endothelial cell migration . In turn, fibronectinrich matrix constitutes an adequate substrate for fibro- The CAM as an in vivo Wound Healing Model· 1075 blasts recruitment, adhesion and differentiation, while the mobilization of fibroblasts is more likely related to tenascin expression 24 • In conclusion, this preliminary study shows that CAM, usually employed as an in vivo model to study angiogenesis 17 can also be utilized as an in vivo WH model. In this respect, then, CAM could allow a very detailed study of angiogenetic kinetics, of the relationship between the latter and the fibroblast intervention, of the different stages in the formation of the inflammatory infiltrate and how it becomes enriched in macrophages, and of the formation of the extracellular matrix. Concerning this latter point, CAM may represent a model for investigating matrix healing, i. e. for neomodeling of collagenic (basement membrane and interstitial) and elastic networks which are probably involved in CAM permeability, strength and plasticity. These studies could be extended to cover the functional activity of the cell populations participating in WH for a better understanding of its physiopathology. Finally, this experimental model may be applied to study neoangiogenesis and competent fibroblasts recruitment modulation in some pathological conditions, i. e. abnormal scarring, tumor associated angiogenesis and fibrosis. Material and Methods The experimental procedures for this study followed the published Guiding Principles in the Care and Use of Animals approved by the Council of the American Physiological Society. Fifty fertilized White Leghorn chick eggs, staged according to Hamburger and Hamilton (HH) 15 were incubated from the start of their embryogenesis in an incubator under of 60% relative humidity at 37 DC. At the HH stage 13, a square window was opened in the egg shell after removing 2-3 ml of albumen in order to detach the developing CAM from the shell. The opening was closed with a glass tape and the incubation continued. In vivo CAM Wound Assay At the HH stage 35, a full thickness excision of a small (1 mm 2 ) area of the CAM devoid of large blood vessels was performed with the aid of a micro knife under a Zeiss SR stereo microscope (Zeiss, Oberkochen, Germany) equipped with the Camera System MC 63. Following removal, the embryos were returned to the incubator. All procedures were performed under sterile conditions. In vivo Stereomicroscopy The stereomicroscope was used to evaluate the CAM vasoproliferative response for up to 96-120 hours after excision. After 96-120 hours (HH stages 39-40) the embryos and their membranes were fixed in vivo in Bouin's fluid. After fixation, the chorioallantoic sacs were isolated from the embryos and dissected in strips, then embedded in paraffin, and serially sectioned at 7 Jlm for microscopy. Assessment of Angiogenic Response Toluidine blue stained sections were used. The angiogenic response of the area close to the excision was evaluated and compared to the angiogenesis of a distant area in the developing CAM, as the normal control. A slightly-modified planimetric point count method 10, 28 was used to evaluate the number of small vessels, i. e. tubes with a single layer of endothelial cells and a diameter of 3-10 Jlm. Briefly, 4 to 6 x 160 fields of every 3rd section (covering almost the whole section) within 30 serial sections from each specimen were analyzed with a 484-intersection point square mesh inserted in the eyepiece of a Leitz Dialux 20 photomicroscope (Leitz, Wetzlar, Germany). The number of vessels was calculated as the number of mesh intersection points which were occupied by the transversally cut vessels, expressed again as a percentage of the total number of intersection points. Immunohistochemistry Fibronectin deposition into the wounds was assessed by using a three-step avidin-biotin-immunoperoxidase as previously described 31 • Briefly, deparaffinized and rehydrated sections exhausted in their endogenous peroxidase with 7.5% H 20 2 were sequentially incubated with: i. an anti-fibronectin murine monoclonal antibody (F3648, Sigma Chemical Co., St. Louis, Mo); ii. a biotin-labeled horse anti-mouse Ig (Vector Inc., Burlingame, CAl, and iii. an avidin-horseradish-peroxidase conjugate (Vector Inc.), red-stained with a 3-amino-9 ethylcarbazole (Sigma) solution, counterstained with Gill's hematoxylin n. 2 (Polyscience Inc., Washington, PAl and mounted in buffered glycerin. Naphthol-AS-D Chloroacetate Esterase Activity After deparaffinization and rehydration, adjacent serial sections were stained for naphthol-AS-D-chloroacetate activity 26 to highlight macrophages. Quantitation of Fibroblasts Fibroblasts were counted in the CAM mesenchyme on 4 to 6 randomly selected x 160 fields of every 3rd section within 30 serial sections from each specimen. The 484-point mesh at x 160 was used, and the number of fibroblasts was calculated as the number of intersection points occupied in the area. Statistical Analysis Means ± 1 standard deviation (SD) were determined for all variables. The statistical significance of the differences between mean values of the intersection points was determined by the Student t-test for unpaired data. Acknowledgements This study was supported in part by grants from the National Research Council, Rome (Progetto Coordinato n. 95.02983.CT14), the Associazione Italiana per la Ricerca sui Cancro (A.I.R.C.), Milan, and the Ministero dell'Universita e della Ricerca Scientifica (60%), Rome, Italy. 1076 . D. Ribatti et al. References 1 Banda WJ, Knighton DR, Hunt TK, Werb Z (1982) Isolation of a non mitogenic angiogenic factor from wound fluid. Proc Nat! Acad Sci USA 79: 7773-7777 2 Broadley KN, Aquino AM, Woodward SC, BuckleySturrock A, Sato Y, Rifkin DB, Davidson JM (1989) Monospecific antibodies implicate basic fibroblast growth factor in normal wound repair. Lab Invest 61: 571-575 3 Broadwell CR, Gospodarowicz D, Nicolson GL (1978) Identification, localization and role of fibronectin in cultured endothelial cells. Proc Nat! Sci USA 75: 3273-3277 4 Buckley A, Davidson JM, Kamerath CD, Wolt TB, Woodward SC (1985) Sustained release of epidermal growth factor accelerates wound repair. Proc Nat! Acad Sci USA 82: 7340-7344 5 Buntrock P, Jentzsch KD, Heder G (1982) Stimulation of wound healing using brain extract with fibroblast growth factor activity. Exp Pathol 21: 46-53 6 Clark RAF, Dvorak HF, Colvin RB(1981) Fibronectin in delayed-type hypersensitivity skin reactions: associations with vessel permeability and endothelial cell activation.J Immunol16: 787-793 7 Clark RA, Della Pelle P, Mansesu E, Lanigan JM, Dvorak HB, Colvin RB (1982) Blood vessel fibronectin increases in conjunction with endothelial cell proliferation and capillary ingrowth during wound healing. J Invest Dermatol 79: 269-276 8 Cohn IK, Diegelman RF, Lindblad WJ (Eds) (1992) Wound Healing: Biochemical and Clinical Aspects W.B. Saunders, Philadelphia-London 9 Edwards LC, Pernokas LN, Dunphy JE(1957) The use of a plastic sponge to sample regeneration in healing wounds. Sur§ Gynecol Obstet 105: 303-309 1 Elias H, Hyde DM(1983) Stereological measurements of isotropic structures. In: Elias H, Hyde DM (Eds) A Guide to Practical Stereology, pp 25 -44. Karger, Basel 11 Folkman J, Brem H(1992) Angiogenesis and inflammation. In: Gallin JI, Goldstein 1M, Snyderman R(Eds) Inflammation, Basic Principles and Clinical Correlates, pp 821839. Raven Press, New York 12 Folkman J, Shing Y (1992) Angiogenesis. J Bioi Chern 267: 10931-10934 13 Gabbiani G, Montandon D (1977) Reparative processes in mammalian wound healing: the role of contractile phenomena. Int Rev Cytol48: 187-219 14 Grinnel F, Billingham RE, Burgess L(1981) Distribution of fibronectin during wound healing in vivo. J Invest Dermatol 76: 181-189 15 Hamburger V, Hamilton HL (1951) A series of normal stages in development of the chick embryo. J Morphol 88: 49-92 16 Knighton DR, Hunt TA, Schenenstuhl H, Halliday BJ, Werb Z, Banda MJ (1983) Oxygen tension regulates the ex- pression of angiogenesis factor by macrophages. Science 221: 1283-1285 17 Knighton DR, Fiegel VD, Philipps GD (1991)The assays of angiogenesis. In: Clinical and Experimental Approaches to Dermal and Epidermal Repair: Normal and Chronic Wounds, pp 291-294. Wiley Liss Inc, New York 18 Kon K, Fujiwara T(1994) Transformation of fibroblasts into endothelial cells during angiogenesis. Cell Tissue Res 278: 625 -628 19 Kurkinen M, Vaheri A, Roberts PJ, Stenman S (1980) Sequential appearance of fibronectin and collagen in experimental granulation tissue. Lab Invest 43: 47-51 20 Kuzuya M, Kinsella JL(1994) Induction of endothelial cell differentiation in vitro by fibroblasts-derived soluble factors. Exp Cell Res 215: 310-318 21 Jaffe EA, Mosher DF (1978) Synthesis of fibronectin by cultured human endothelial cells. J Exp Med 147: 17791791 22 Leibovich SJ, Wiseman DM (1988) Macrophages, wound repair and angiogenesis. In: Growth Factors and Other Aspects of Wound Healing: Biological and Clinical Implications, pp 131-145. Alan R Liss Inc, New York 23 Linch SE, Colvin RB, Antoniades HN (1989) Growth factors in wound healing: single and synergistic effects on partial thickness porcine wounds. J Clin Invest 84: 640-646 24 Mackie EJ, Halfter W, Liverani D (1988) Induction of tenascin in healing wounds J Cell Bioi 107: 2757-2767 25 Mc Grath MH, Emery JMI (1985) The effect of inhibition of angiogenesis in granulation tissue on wound healing and the fibroblast. Ann Plast Surg 15: 106-119 26 Moloney WC, Mc Pherson K, Fliegelman L (1960) Esterase activity in leucocytes demonstrated by the use of naphthol AS-D-chloroacetate substrate. J Histochem Cytochern 8: 200-207 27 Murphy-Ulrich JE, Mosher DF(1986) Fibronectin and disease processes. In: Vitto J, Perejda AJ(Eds) Connective Tissue Disease: Molecular Pathology of the Extracellular Matrix, pp. 455-473. Marcel Dekker Inc, New York 28 Ribatti D, Vacca A, Bertossi M, de Benedictis G, Roncali L, Dammacco F (1990) Angiogenesis induced by B-cell nonHodgkin's lymphomas. Lack of correlation with tumor malignancy and immunologic phenotype. Anticancer Res 10: 401406 29 Ribatti D, Urbinati C, Nico B, Rusnati M, Roncali L, Presta M (1995) Endogenous basic fibroblast growth factor is implicated in the vascularization of the chick embryo chorioallantoic membrane. Dev Bioi 170: 39-49 30 Sunderkotter C, Steinbrink K, Goebeler M, Bhardwai R, Sorg C (1994) Macrophages and angiogenesis. J Leukoc Bioi 55: 410-422 31 Vacca A, Ribatti D, Roncali L, Ranieri G, Serio G, Silvestris F, Dammacco F(1994) Bone marrow angiogenesis and progression in multiple myeloma. Brit J Haematol 87: 503508 Received August 11, 1995. Accepted in revised form April 19, 1996 Key words: Chorioallantoic membrane - Chick embryo - Wound healing.;.. Angiogenesis Ribatti, MI?, ~n~titute of Human Anatomy, Histology and Embryology, University of Bari Medical School, Piazza GUlllO Cesare, 11, Pohchmco, 1-70124 Bari, Italy, Telephone: 0039.80.5473569, Telefax. 0039.80.5478309 Do~enico